Page 1 of 1
3Month-Old Boy With Severe Failure to Thrive & Hypercalcemia
Posted: 19 May 2010, 20:23
by Hani

A 3-month-old white male infant is presented to the pediatric clinic for a routine well-child examination and care. The birth and perinatal history include a spontaneous vaginal delivery at term to a G3 P2 31-year-old woman with normal prenatal sonograms and excellent prenatal care. The prenatal history was uneventful. Upon circumcision at age 4 days, he experienced a choking spell after being restrained, but he recovered without further incident. He has been breast-feeding since being discharged from the hospital, and at that time he weighed 2.9kg (6 lb 7 oz). Upon follow-up, he had normal oxygen saturation and his weight was up to 3.04kg (6 lb 12 oz) at his 2-week examination. There is no significant family history. He is not currently on any medications and there is no history of any known allergies.
On examination, the baby, although smiling, appears to be severely malnourished. He has an absence of subcutaneous fat, and his skin appears wrinkled and tented. He does not seem to be in any acute distress. His vital signs include a pulse of 130 bpm, respiratory rate of 28 breaths/min, temperature of 98.2° F (36.8° C), and blood pressure of 127/71 mm Hg. His weight is 2.84kg (6 lb 5 oz), which is below the 3rd percentile for an infant of this age, and he is measured at 21 in long, which also falls below the 3rd percentile for his age. His head circumference is 14.75 in (also below the 3rd percentile). He weighs less now than he did at birth. His abdomen appears bloated, but there is no evidence of any organomegaly. The heart and lung examinations are normal. Further examination reveals apparently normal hearing and sight. According to the parents, the baby only takes about 7 oz of baby formula per day (approximately 0.5-1 oz of formula every 2-3 hours and 0.5-1 oz of breast milk per day). The patient cries when feeding in the office. The child's mother has switched him to a low-flow nipple as a precaution against choking. The patient is admitted for 10 days in the hospital. When examined afterwards, the patient is found to still have no appetite, continues to cry when feeding (although his weight has increased to 8 lb), and appears more hypoxic than normal babies.
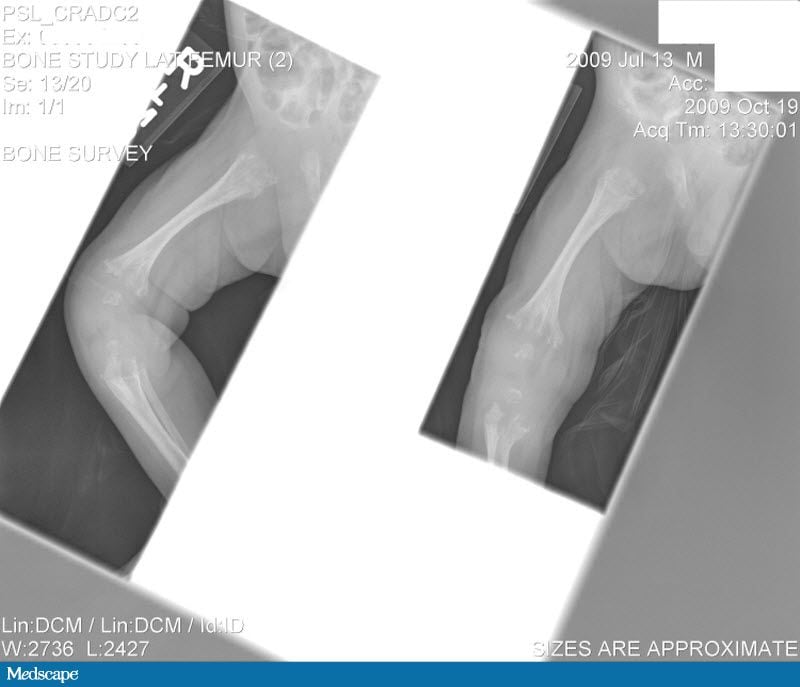
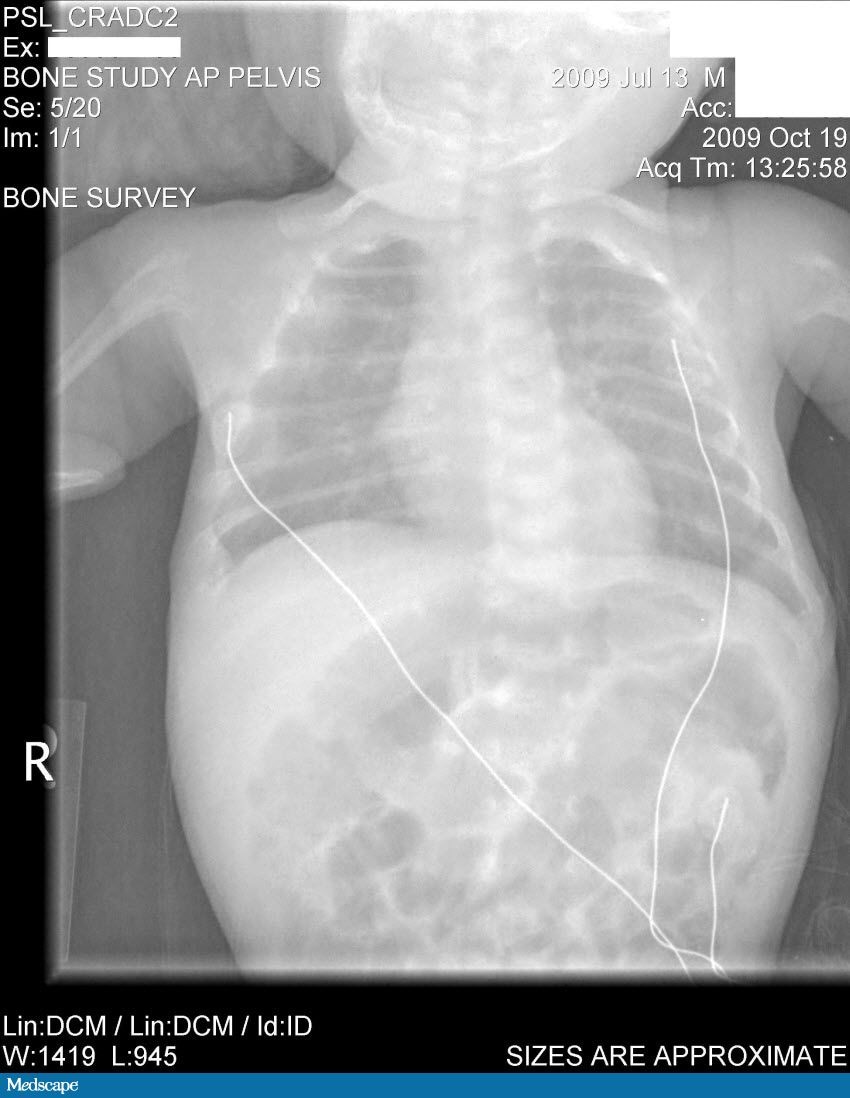
Laboratory tests done at the time of hospitalization show that the patient has severe hypercalcemia, with a total calcium of 18.1 mg/dL (normal range, 9-10.5 mg/dL) and an ionized calcium of 8.8 mg/dL. He also has a low normal phosphate of 4.4-4.5 mg/dL. The alkaline phosphatase level is 93 mg/dL (normal range, 143-320 mg/dL). His urine phosphoethanolamine level is 2142 nmol/mg of creatinine, and his vitamin B6 level is >100 µg/dL. A 2-dimensional echocardiogram is normal; however, a radiographic inspection of his bone quality reveals irregular metaphyses, along with severe metaphyseal flaring and osteopenia. A renal ultrasound reveals bilateral hydronephrosis that is moderate on the left and mild on the right. There is also a possibility of an obstruction at the uretero-pelvic junction on the left, with a milder obstruction on the right. A voiding cystourethrogram (VCUG) is negative. The patient's oxygen saturation is 72%-76% on room air; however, this measurement is obtained at his home, which is at an elevation of 10,000 feet.
Hint: Keep in mind the severe hypercalcemia, alkaline phosphatase, and radiology results.
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 18:42
by khalafalla
Thanks Dr.Hani for sharing us with this problem. I want to go step by step in order to reach the final diagnosis. May be my answer will be wrong but just let us make a try.
----------
First we have to extract the positive findings and relevant information provided:
Age: 3 yrs old
Sex: Male
Ethinicity: White (important because some diseases occurs more in black and others occur more in white)
C/O: no appetite, CHOKING, Cry during breast feeding
O/E: severely malnourished, an absence of subcutaneous fat, and his skin appears wrinkled and tented.
Wt: 2.84kg ----below the 3rd percentile for an infant of this age
Height: 21 in-----below the 3rd percentile for an infant of this age
Head circumference:14.75 in-----below the 3rd percentile for an infant of this age
Laboratory investigations:
a total calcium of 18.1 mg/dL (normal range, 9-10.5 mg/dL)
a low normal phosphate of 4.4-4.5 mg/dL
The alkaline phosphatase level is 93 mg/dL (normal range, 143-320 mg/dL)
X-ray Bone:
irregular metaphyses, along with severe metaphyseal flaring and osteopenia.
Renal US:
bilateral hydronephrosis
a possibility of an obstruction at the uretero-pelvic junction
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 18:45
by khalafalla
Second step in solving this problem is revising the metabolism of calcium:

Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 18:49
by khalafalla
-----------------------------------------------
Calcium Balance
Maintenance of serum calcium levels within a narrow range is vital for normal functioning of the nervous system, as well as for bone growth, and maintenance of bone density. Vitamin D is essential for the efficient utilization of calcium by the body (1). The parathyroid glands sense serum calcium levels, and secrete parathyroid hormone (PTH) if calcium levels drop too low. Elevations in PTH increase the activity of 25(OH)D3-1-hydroxylase enzyme in the kidney, resulting in increased production of 1,25(OH)2D. Increasing 1,25(OH)2D production results in changes in gene expression that normalize serum calcium by 1) increasing the intestinal absorption of dietary calcium, 2) increasing the reabsorption of calcium filtered by the kidneys and 3) mobilizing calcium from bone when there is insufficient dietary calcium to maintain normal serum calcium levels. Parathyroid hormone and 1,25(OH)2D are required for the latter two effects
----------------------------
The source of the above information is:
http://www.google.com
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 18:52
by khalafalla

I have to go now..I will continue tomorrow
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 19:15
by khalafalla
Regarding hypercalcemia we have to remember the following:
The ionized calcium concentration, not the total calcium concentration, is physiologically relevant. Hypercalcemia may go undetected in the patient with hypoalbuminemia and a “normal” total calcium concentration. The ionized calcium concentration is the gold standard for evaluating children with calcium disorders.
Nelson Textbook of Pediatrics
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 19:29
by khalafalla
Causes of Hypercalcemia:
EXCESS PARATHYROID HORMONE
Primary hyperparathyroidism
Sporadic adenoma
Familial isolated hyperparathyroidism
Multiple endocrine neoplasia type I
Multiple endocrine neoplasia type II
Hyperparathyroidism–jaw tumor syndrome
Calcium-sensing receptor mutation
Transient secondary neonatal hyperparathyroidism
Tertiary hyperparathyroidism
EXCESS VITAMIN D
Hypervitaminosis D
Subcutaneous fat necrosis
Sarcoidosis
Granulomatous diseases (e.g., tuberculosis and fungal infections)
Lymphomas
EXCESS CALCIUM INTAKE
Calcium supplements
Iatrogenic (e.g., total parenteral nutrition)
EXCESS RENAL REABSORPTION OF CALCIUM
Familial benign hypocalciuric hypercalcemia
Thiazide diuretics
RELEASE FROM BONE
Thyrotoxicosis
Hypervitaminosis A
Malignancy associated
Ectopic parathyroid hormone (PTH)
PTH-related peptide
Bone metastasis
Other factors
Immobilization
Renal osteodystrophy
Low turnover disease
Aluminum deposition
MISCELLANEOUS
Williams syndrome
Hypophosphatemia
Pheochromocytoma
Adrenal insufficiency
Recovery phase of rhabdomyolysis
Jansen metaphyseal chondrodysplasia
Hypophosphatasia
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 20:01
by khalafalla
Osteopenia is a decrease in the amount of calcium and phosphorus in the bone. This can cause bones to be weak and brittle, and increases the risk for broken bones.
The source
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 20:20
by khalafalla
Alkaline phosphatase (ALP) is a hydrolase enzyme responsible for removing phosphate groups from many types of molecules, including nucleotides, proteins, and alkaloids. The process of removing the phosphate group is called dephosphorylation. As the name suggests, alkaline phosphatases are most effective in an alkaline environment. It is sometimes used synonymously as basic phosphatase.(1)
Elevated ALP indicates that there could be active bone deposition occurring as ALP is a by product of osteoblast activity (such as the case in Paget's disease of bone).
----------
Reference:
1- Tamás L, Huttová J, Mistrk I, Kogan G (2002). "Effect of Carboxymethyl Chitin-Glucan on the Activity of Some Hydrolytic Enzymes in Maize Plants". Chem. Pap. 56 (5): 326–329.
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 20 May 2010, 20:22
by khalafalla
The following conditions or diseases may lead to reduced levels of alkaline phosphatase:
Hypophosphatasia, an autosomal recessive disease
Postmenopausal women receiving estrogen therapy because of osteoporosis
Men with recent heart surgery, malnutrition, magnesium deficiency, hypothyroidism or severe anemia
Children with achondroplasia and cretinism
Children after a severe episode of enteritis
Pernicious anemia
Aplastic anemia
Chronic myelogenous leukemia
----
Wiki
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 21 May 2010, 10:49
by khalafalla
Also to understand the condition of this child we have to put some light on basics of bone metabolism:

Parathyroid hormone receptors are found on osteoblasts. Parathyroid hormone (PTH) stimulation of osteoblasts increases osteoblast production of receptor activator of nuclear factor kappa-B ligand (RANKL). Hematopoietic cell precursors stimulated by M-CSF give rise to osteoclasts that express RANK receptor. The RANKL/RANK interaction stimulates differentation of the osteoclasts so that they can resorb bone. Osteoblasts also produce a decoy receptor called osteoprotegerin (OPG) that binds to RANKL and prevents the RANKL/RANK interaction.
Estradiol increases production of OPG to diminish bone resorption. Glucocorticoids stimulate RANKL expression while inhibiting OPG synthesis by osteoblasts to enhance osteoclast proliferation and differentiation, leading to bone resorption.
library.med.utah.edu
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 21 May 2010, 10:57
by khalafalla
Bilateral hydronephrosis result of possible stones is something secondary to hypercalcemia. The same issue regarding the poor breast feeding and failure to thrive are all related to hypercalcemia. So the primary lesion produce hypercalcemia, low alkaline phosaphatase and osteopenia. Putting these three imortant findings together and search of a disease which lead to them is the cornerstone to reach the diagnosis.

Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 23 Jul 2010, 17:12
by Dr.Sudan
Thanks Dr.Khalafallah ... extraordinary explanation ...
many thanks
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 05 Sep 2013, 09:17
by mohamedhakem
THAK YOU Dr Khafalla
Re: 3Month-Old Boy With Severe Failure to Thrive & Hypercalc
Posted: 05 Sep 2013, 09:52
by mohamedhakem
Hypophosphatasia, especially the severe infantile form, is usually associated with mild to moderate hypercalcemia (see Chapter 694 ). Serum levels of phosphorus are
normal, and those of alkaline phosphatase are subnormal. The bones exhibit rachitic-like lesions on radiographs. Urinary levels of phosphoethanolamine, inorganic
pyrophosphate, and pyridoxal 5'-phosphate are elevated; each is a natural substrate to a tissue-nonspecific (liver, bone, kidney) alkaline phosphatase enzyme.
Missense mutations of the tissue-nonspecific alkaline phosphatase enzyme gene result in an inactive enzyme in this autosomal recessive disorder.
from nelson17ed