


A 3-month-old white male infant is presented to the pediatric clinic for a routine well-child examination and care. The birth and perinatal history include a spontaneous vaginal delivery at term to a G3 P2 31-year-old woman with normal prenatal sonograms and excellent prenatal care. The prenatal history was uneventful. Upon circumcision at age 4 days, he experienced a choking spell after being restrained, but he recovered without further incident. He has been breast-feeding since being discharged from the hospital, and at that time he weighed 2.9kg (6 lb 7 oz). Upon follow-up, he had normal oxygen saturation and his weight was up to 3.04kg (6 lb 12 oz) at his 2-week examination. There is no significant family history. He is not currently on any medications and there is no history of any known allergies.
On examination, the baby, although smiling, appears to be severely malnourished. He has an absence of subcutaneous fat, and his skin appears wrinkled and tented. He does not seem to be in any acute distress. His vital signs include a pulse of 130 bpm, respiratory rate of 28 breaths/min, temperature of 98.2° F (36.8° C), and blood pressure of 127/71 mm Hg. His weight is 2.84kg (6 lb 5 oz), which is below the 3rd percentile for an infant of this age, and he is measured at 21 in long, which also falls below the 3rd percentile for his age. His head circumference is 14.75 in (also below the 3rd percentile). He weighs less now than he did at birth. His abdomen appears bloated, but there is no evidence of any organomegaly. The heart and lung examinations are normal. Further examination reveals apparently normal hearing and sight. According to the parents, the baby only takes about 7 oz of baby formula per day (approximately 0.5-1 oz of formula every 2-3 hours and 0.5-1 oz of breast milk per day). The patient cries when feeding in the office. The child's mother has switched him to a low-flow nipple as a precaution against choking. The patient is admitted for 10 days in the hospital. When examined afterwards, the patient is found to still have no appetite, continues to cry when feeding (although his weight has increased to 8 lb), and appears more hypoxic than normal babies.
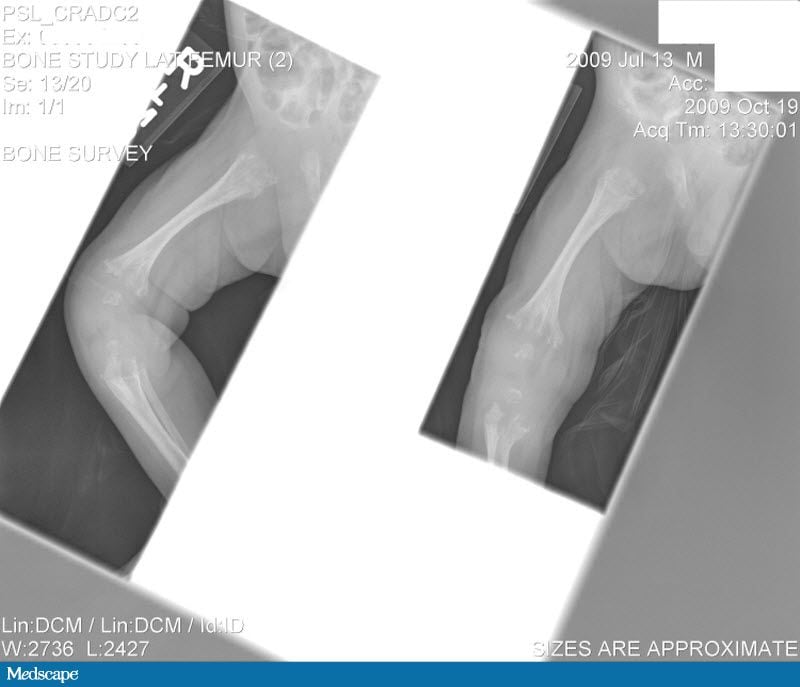
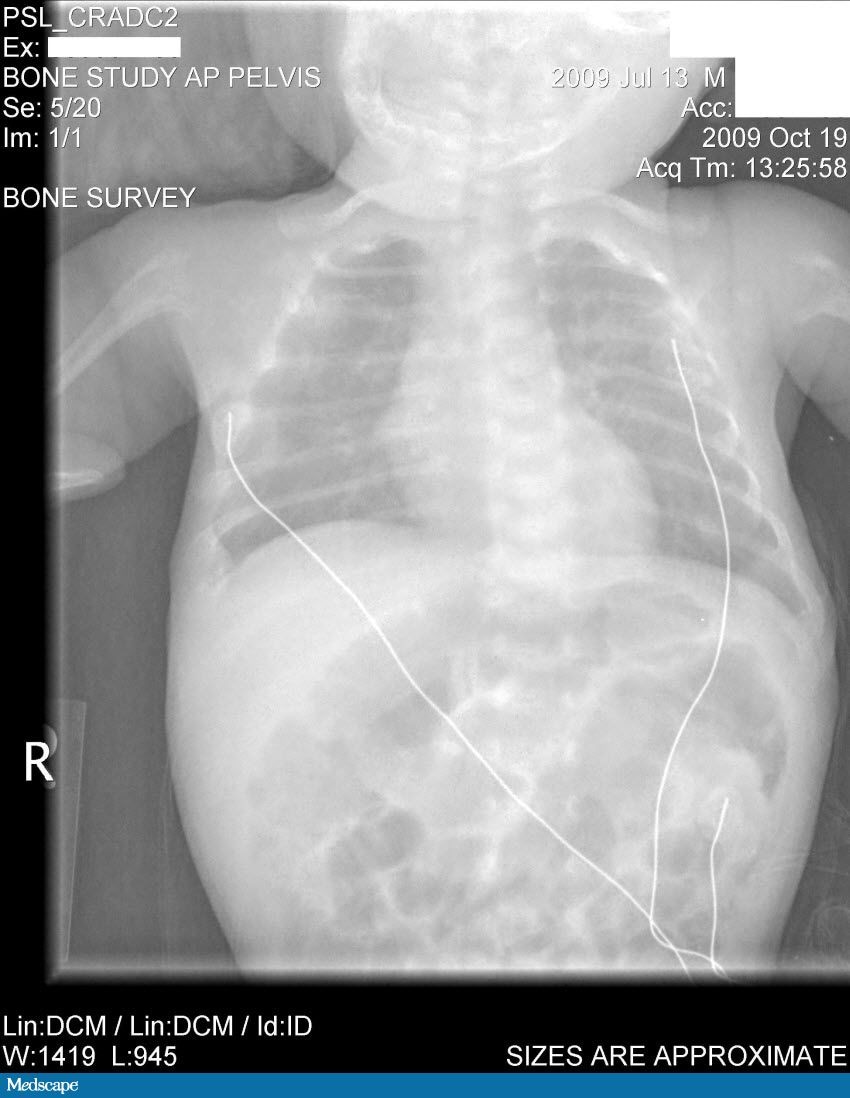
Laboratory tests done at the time of hospitalization show that the patient has severe hypercalcemia, with a total calcium of 18.1 mg/dL (normal range, 9-10.5 mg/dL) and an ionized calcium of 8.8 mg/dL. He also has a low normal phosphate of 4.4-4.5 mg/dL. The alkaline phosphatase level is 93 mg/dL (normal range, 143-320 mg/dL). His urine phosphoethanolamine level is 2142 nmol/mg of creatinine, and his vitamin B6 level is >100 µg/dL. A 2-dimensional echocardiogram is normal; however, a radiographic inspection of his bone quality reveals irregular metaphyses, along with severe metaphyseal flaring and osteopenia. A renal ultrasound reveals bilateral hydronephrosis that is moderate on the left and mild on the right. There is also a possibility of an obstruction at the uretero-pelvic junction on the left, with a milder obstruction on the right. A voiding cystourethrogram (VCUG) is negative. The patient's oxygen saturation is 72%-76% on room air; however, this measurement is obtained at his home, which is at an elevation of 10,000 feet.
Hint: Keep in mind the severe hypercalcemia, alkaline phosphatase, and radiology results.





